
Understanding SIBO: When Gut Bacteria Go Rogue
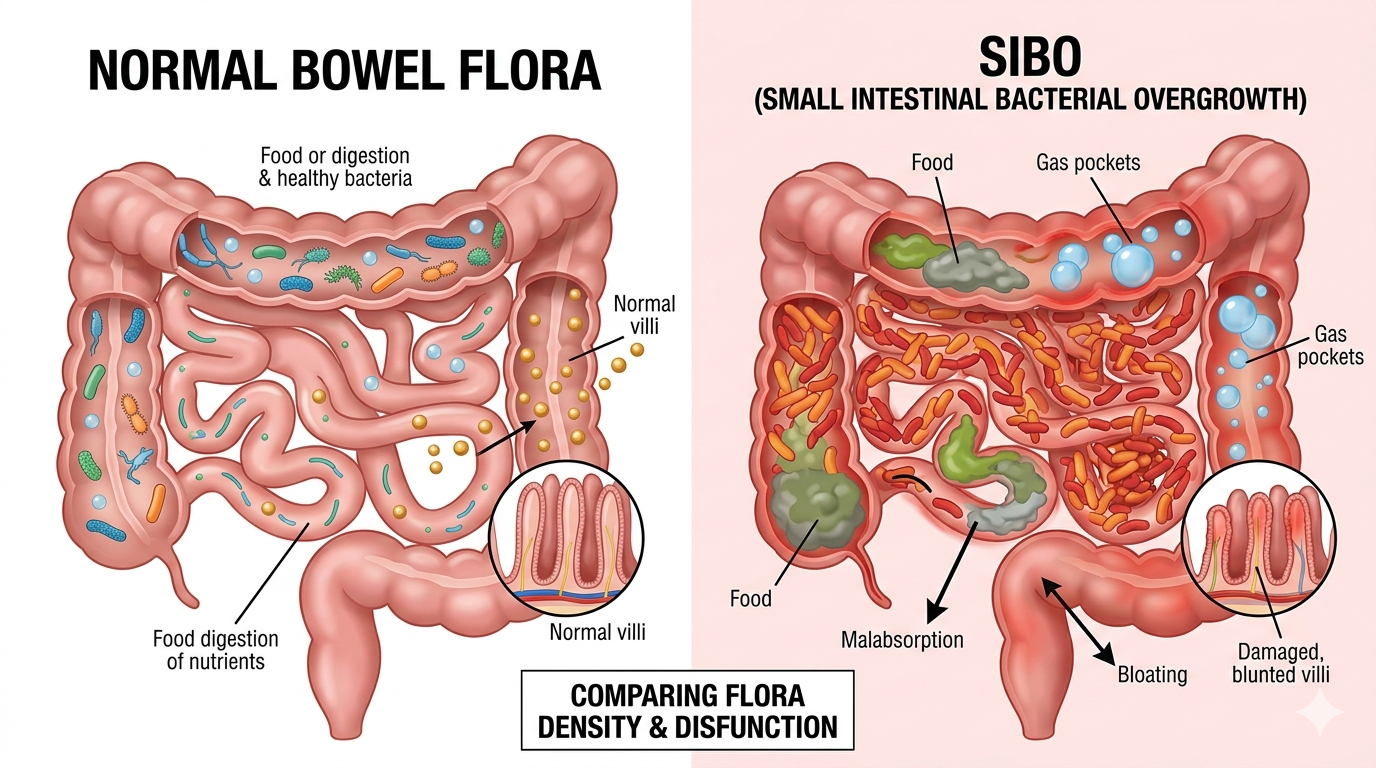
The human gut microbiome is a complex and dynamic ecosystem, made up of trillions of bacteria that play a central role in digestion, immune regulation, metabolism, and even brain function. In a healthy digestive system, these microorganisms are carefully distributed—relatively low in the stomach and small intestine, and highly concentrated in the large intestine.
This balance is not accidental. The small intestine is designed primarily for digestion and nutrient absorption, and several protective mechanisms, including stomach acid, digestive enzymes, and coordinated gut motility, help keep bacterial levels under control.
SIBO (Small Intestinal Bacterial Overgrowth) develops when these protective mechanisms are disrupted. As a result, bacteria begin to accumulate in the small intestine, where they ferment carbohydrates prematurely, producing gases such as hydrogen and methane. This process can lead to symptoms including bloating, abdominal distension, excess gas, diarrhoea or constipation, and, in some cases, fatigue and brain fog.
SIBO is increasingly recognised as a significant contributor to chronic digestive symptoms, particularly in individuals diagnosed with irritable bowel syndrome (IBS). Studies suggest that up to 40–70% of IBS patients may have underlying SIBO, highlighting a substantial overlap between the two conditions.
Despite growing awareness, SIBO remains underdiagnosed in routine clinical practice. Many patients are treated symptomatically without investigation into the underlying cause, which may explain why symptoms often persist or recur over time.
Why Does SIBO Develop?
SIBO rarely occurs without an underlying trigger. In most cases, it develops when normal mechanisms that regulate digestion and bacterial balance are disrupted over time.
One of the most important factors is impaired gut motility. The small intestine relies on coordinated movements (the migrating motor complex) to clear food and bacteria between meals. When this process is slowed—due to stress, inflammation, or certain medications—bacteria are more likely to accumulate.
Several well-recognised risk factors have been identified:
Long-term use of acid-suppressing medication (PPIs)
Reduced stomach acid can weaken one of the body’s primary defences against bacterial overgrowth. Studies have shown an increased prevalence of SIBO in individuals taking proton pump inhibitors.Frequent or repeated antibiotic use
Antibiotics can disrupt the balance of the gut microbiome, sometimes leading to longer-term dysbiosis and altered bacterial distribution.Medications that affect gut motility
Opiate-based medications (including morphine derivatives) are known to slow intestinal transit and are associated with a higher risk of bacterial overgrowth.Dietary patterns
Diets high in refined carbohydrates and frequent snacking may promote ongoing fermentation and reduce the natural “cleansing waves” of the gut. Conversely, highly restrictive diets or a history of disordered eating may impair digestive function over time.Chronic stress
Stress can affect both gut motility and digestive secretions, altering the environment within the small intestine and increasing susceptibility to imbalance.
SIBO is therefore best understood not as an isolated condition, but as the result of cumulative disruption to normal digestive physiology. SIBO, they reflect the broader impact that gut dysfunction can have on overall health.SIBO and the Wider Gut–Brain Connection
Gas Production in the Gut and Its Role
Gas production is a normal part of digestion. As bacteria break down food, particularly carbohydrates, they produce gases such as hydrogen, methane, and carbon dioxide.
In a healthy digestive system, this process occurs mainly in the large intestine, and most of the gas produced is either absorbed into the bloodstream or expelled without causing significant symptoms.
In SIBO, however, this fermentation takes place earlier in the small intestine, where it does not normally occur to the same extent. This can lead to an excessive and misplaced accumulation of gas, contributing to symptoms such as bloating, abdominal distension, discomfort, and altered bowel habits. In some cases, the pressure from excess gas may also be experienced as upper abdominal or even chest discomfort.
A key feature of SIBO is the type of gas produced. Hydrogen is more commonly associated with diarrhoea, while methane is linked to slower gut motility and constipation. Some individuals may produce a combination of both, leading to mixed or fluctuating symptoms.
These gases are not only responsible for symptoms—they are also central to diagnosis.
Breath testing works by measuring hydrogen and methane levels in exhaled air after ingestion of a test substrate. As these gases are absorbed into the bloodstream and transported to the lungs, they can provide a useful, non-invasive indication of bacterial overgrowth in the small intestine.
Treatment Approaches: Why Structure Matters
There is no single treatment for SIBO that works for everyone. Effective management usually involves combining several approaches, tailored to the individual. Antimicrobial therapy, either with antibiotics or carefully selected herbal protocols, can help reduce bacterial overgrowth. However, response varies, and recurrence is common if treatment is not part of a broader plan.
Supporting gut motility is equally important. If the natural movement of the small intestine remains impaired, bacteria can reaccumulate over time. This is one of the key reasons why treatment may only provide temporary relief if underlying factors are not addressed.
The role of probiotics is more complex.
Some individuals benefit, while others find that symptoms worsen, particularly in the early stages. For this reason, their use needs to be individualised rather than routine. Overall, the most consistent clinical observation is that structured, phased treatment tends to be more effective than relying on a single intervention.
The Role of Diet
Diet can have a significant impact on symptoms, particularly by influencing fermentation within the gut. Reducing fermentable carbohydrates (for example, through a low FODMAP-style approach) may help alleviate bloating and discomfort in the short term. However, dietary restriction alone is rarely sufficient to resolve SIBO and is not intended as a long-term strategy.
Many individuals benefit from a more structured approach to eating patterns, such as allowing time between meals to support gut motility, identifying specific trigger foods, and adjusting portion sizes. Importantly, overly restrictive diets can be counterproductive if maintained long term, potentially affecting nutritional status and the diversity of the microbiome.
Understanding and Managing Relapse
Relapse is a recognised feature of SIBO and can occur even after initial improvement.
Common triggers include periods of stress, intercurrent illness, dietary changes, or a return of underlying issues such as impaired gut motility. This reflects the fact that SIBO is often a consequence of broader physiological disruption rather than an isolated condition.
In practice, it can be helpful to recognise early patterns, such as the return of post-meal bloating or food sensitivities and to respond in a structured way. A clear plan, tailored to the individual, often allows symptoms to be managed more effectively and reduces the need for repeated or reactive treatment.